
CC: Vomiting for 2 days
HPI: 47 year old female with PMHX of HTN and ETOH abuse presents with abdominal pain. Patient states that beginning two days ago she was woken up from her sleep with sudden onset non-bloody vomiting as well as epigastric pain which radiates to the back and is sharp in nature. She admits to over 15 episodes of vomiting. She is also having cramping of her feet bilaterally. She admits to daily ETOH use, and states her last intake was two days ago, denies illicit drug use. Denies taking any medication prior to arrival. Denies fever, chills, chest pain, SOB or dysuria. Denies recent travel or sick contacts. PMHX/PSHX: none Meds: none Allergies: none
Physical Exam: Vitals: BP 150/96 P 98 RR 16 O2 sat 98% RA General: Awake, alert, anxious Cardiac: Regular rate, no murmurs Lungs: CTAB, no rales, no rhonchi, no wheezing Abd: soft, non-distended, Mild tenderness to palpation epigastric area
Labs: Magnesium- 1.3 Potassium- 3.5 Troponin- 0.017
EKG:
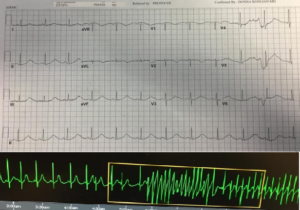
DX: Prolonged QT interval with non-sustained polymorphic Ventricular tachycardia secondary to Hypomagnesemia
ED/Hospital course: Upon arrival to ED patient had Epigastric pain with vomiting, Patient started on IVF and received Pepcid and Zofran. EKG at this time showed QT prolongation and patient found to have magnesium of 1.3. While waiting for magnesium, she started to have short runs of polymorphic ventricular tachycardia and during these times she complained of chest tightness. After 2 grams of magnesium patients repeat EKG showed normal QT and runs of ventricular tachycardia stopped. She received another 2mg of Magnesium and 40 mEq of Potassium Chloride. Patient was then admitted to Telemetry floor. Patient observed for 24hours and discharged to home with follow up with a cardiologist and Norvasc 5 mg 1tab PO daily, Losartan 100 mg 1tab PO daily, Ranitidine 150mg 1tab PO BI.
Pearls:
- An abnormally prolonged QTc, especially >500 is associated with an increased risk of ventricular arrhythmias, Torsade’s de Pointes
- Prolonged QT with prolonged T wave is due to: HypoK, HypoMg, Medications, Elevated ICP, Cardiac ischemia, Congenital.
- Prolonged QT with prolonged ST-segment is due to: HypoCa, Hypothermia.
- If EKG reveals long QT start by reviewing drug history and checking electrolytes. Stop any offending agents. Suppress early after depolarization with IV magnesium sulfate and keep potassium >4.5meq/L.
- If non responsive to magnesium, may consider cardiac pacing and rarely isoproterenol infusion. Acceleration of the heart rate may produce suppression of arrhythmias, with a reduction in the QT interval.
- Unstable patients should undergo non-synchronized electrical defibrillation.
Post by: Dr. Kerri Clayton, DO