CC: Hand Injury-Job Related
HPI: 35 yo otherwise healthy male presents to the Emergency Dept. (ED) with a laceration over the palmar surface of the left hand, proximal to the PIP joint and extending over the MCP joints of the 4th and 5th digit. He sustained this injury at work one hour ago. He is a firefighter and was responding to a house fire when he accidently tripped over an object in a smoke filled room while putting on his glove. He states his left hand went through a glass door. At the scene, patient washed it out with sterile saline and a dressing was applied. Pt also complaints of decreased sensation to the distal aspect of his left 5th digit. He denies any other trauma, preceding symptoms of chest pain, dizziness, feeling lightheaded, palpitations, inhalation injury or difficulty breathing. Denies head injury, neck pain or LOC. Last tetanus is unknown.
Physical Exam:
Vitals: BP 155/97 Pulse 97 RR 15 T 98.6F SpO2 100% on RA
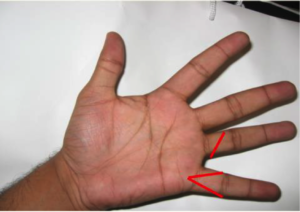
MSK/extremities: 2.5cm complex “V” shaped laceration over the palmar MCP of the left 5th digit that is oozing blood; no arterial bleeding noted. Tissue flap noted. 1.5 cm laceration over the left palmar aspect of the 4th digit between the MCP and PIP joint. Hemostasis noted. Small tissue flap noted. Sensation intact over the distal left 4th digit; Sensation mildly decreased over the distal left 5th digit. Cap refill brisk both digits. Pt is able to flex and extend both digits.
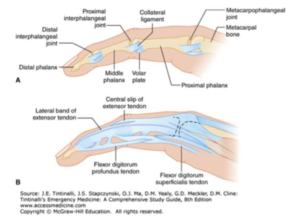
Location of laceration
:
Pertinent Labs (if any): N/A
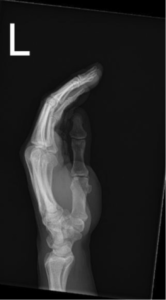
Pertinent Imaging/EKG: No displaced fracture or dislocation. No radiopaque foreign body is identified.


Working Diagnosis: Prior to x-rays: possible FB, dislocation/subluxation, fracture. Possible Partial flexor tendon laceration.
ED/Hospital course: Pt received Toradol for pain and a tetanus shot
- Digital block was performed on the 4th and 5th digits of the left hand by injecting lidocaine into the web spaces as well as local was performed on the palm where the digital block was ineffective.
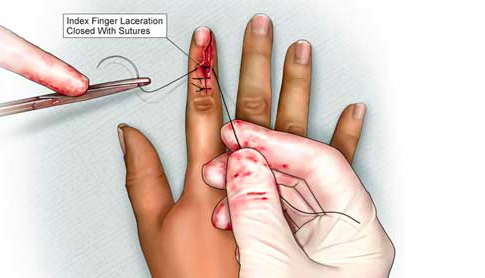
- Moderate bleeding/oozing noted of the 5th left finger laceration. Upon lifting the tissue flap of the 5th digit the flexor tendon was exposed but not lacerated. The 4th left digit wound more superficial. No tendon exposed. No FB found in either laceration.
- 4th finger closed w/ six 4-0 Ethilon sutures
- 5th finger closed w/ ten 4-0 Ethilon sutures
- Pt discharged w/ Rx for: Bacitracin Ibuprofen Keflex F/u w/ employee health F/u in 7-10 days for suture removal
Pearls & Takeaways:
- For lacerations to the hand or other injuries that may or may not involve a tendon always ask:
- Position of hand injury?
- Crush, burn, injection, chemical injury?
- Other trauma or preceding symptoms?
- Exam for hand/wrist lacerations
- Check and compare Bilateral grip strength
- Check sensation
- Compare bilaterally with 2 point discrimination to the volar aspect of each fingertip
- Normal 2 point discrimination on the hand is 5-6 mm
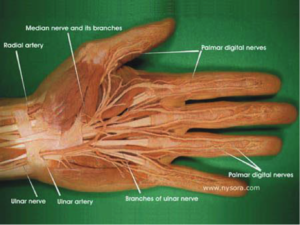
- Review of nerve distribution :
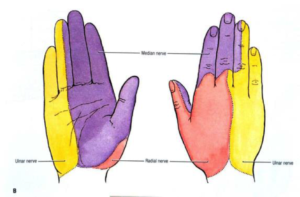
- Check Motor function
- Ask them to make a clenched fist— The middle and distal phalanges should all be parallel to each other with the nails positioned in the same plane and pointing toward the Scaphoid when fist is clenched
- Ulnar Nerve innervates the Lumbricals and Adductor Pollices Muscles
- Lumbricals: Have patient abduct their fingers and have them resist the force of you pushing their fingers back to midline
- Adductor Pollices Test: Have patient hold a piece of paper with the volar pulp of the thumb and PIP of index finger. If you pull away at the paper, and pt is able to maintain the key pinch of paper against resistance then adductor pollicis is strong.
- Look for Froment’s Sign ( Flexes IP joint of thumb to compensate for weak Adductor Pollices)
- https://www.youtube.com/watch?v=yJTIhm1VfSI
- Median Nerve
- Make the “OK” Sign (Flexor Pollicus Longus)
- Opposition (Thenar Muscles): As them to touch their pinky with their thumb
- Ask pt to abduct their thumb with palm up and have the pt resist a force to redirect the thumb toward the palm (Abductor Pollicis longus)
- Radial Nerve
- With palm on the table, hyperextend all fingers against resistance from can have them lay their palm flat on a table, and lift each digit straight up and extend up from the table while keeping the palm flat
- Vascular
- Check for capillary refill and pulses
- Flexor Tendor Testing
- 90% of the tendon can be severed/lacerated with preservation of ROM without RESISTANCE.
- Apply resistance when testing for tendon function
- Pain along course of tendon during resistance testing suggest partial laceration even if pt has FULL ROM
- Test for Flexor Digitalis Profundus (FDP): Ask the to flex their DIP joint against resistance while holding their MCP and PIP joint in extension
- Test for Flexor Digitalis Superficialis (FDS): Ask to flex their PIP joint against resistance while ALL the rest of the fingers are held in full extension (Hyperextension disengages FDP and the FDS function is isolated).
- Imaging
- If isolated fingers involved, get a AP, oblique and lateral view of the designated finger as well as the hand
- Digital Blocks
- Web Space– Inject 1-3 mL of Anesthetic
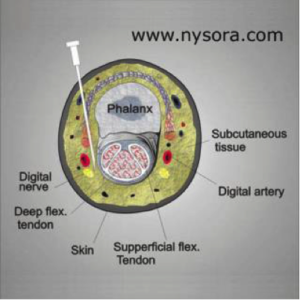
- Transthecal
- Inject into flexor Tendon sheath
- ID distal palmar crease and tendon
- Insert needle at 45 degrees just distal to crease
- Inject
- If resistance, withdraw slightly
- Apply proximal pressure
- Pros: Only 1 poke and numbs entire finger
- Cons: It’s over most sensitive part of the hand

- Method to get a bloodless field
- Use tourniquet or Penrose drain at base of finger secured by hemostat
- Use another tourniquet or gauze to wrap around distal end of finger and wrap w/ moderate compression down from most distal part to laceration milking out the blood in the distal finger
- Do not leave tourniquet on for >20 minutes
- What If there is a stellate laceration?
- Great video on the corner stitch! Try it next time!
- https://lacerationrepair.com/techniques/basic-suturing-techniques/the-corner-stitch/
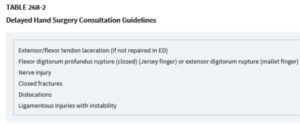
- When to refer tendon lacerations:
- Splinting tendon Injuries:
- General rule is to splint in the direction of function
- Extensor tendons splinted in extension
- Flexor tendons splinted in flexion
- Flexor Tendon Injuries specifically:
- Dorsal splint
- Wrist flexed to 30 degrees
- 70 degree MCP flexion
- 30-45 degree PIP flexion

- Antibiotics
- NO Great guidelines
- ACEP Clinical guidelines
- Looks ok-à No ABX
- Looks bad-à ABX
- If simple laceration -à no ABX
- If not simple (contaminated, infected, bone, tendon, joint involvement)-à ABX
- 1st line: Cephalosporin
- Consider Context:
- Human, Cat, Dog Bites: Amoxicilin/Clavulanic Acid (Augmentin)
- Open fractures: Cefazolin (Ancef)
- Visibly dirty and open wound: Ancef + Gentamycin
- General rule is to splint in the direction of function
Case presented by Dr. Jessica Williams