Presenting Resident: Katrina D’Amore, PGY4
Chief Complaint: Palpitations
Brief HPI: 36 y/o F G4P2012 at 18 weeks gestation presents complaining of palpitations that began this morning. Patient reports a history of “SVT” multiple times in the past and she even underwent ablation in 2012. Patient states that “Adenosine never ever works for me.” Patient denies any other symptoms and was in her usual state of health until the symptoms began this morning. Patient does report she was recently
started on Synthroid by her OB for subclinical hypothyroidism.
Pertinent PE and Vitals
VS: Afebrile, HR 203 bpm, BP 125/86, 98% on RA
Patient appears uncomfortable but not in distress. PE unremarkable except for tachycardia.
Pertinent Imaging/EKG
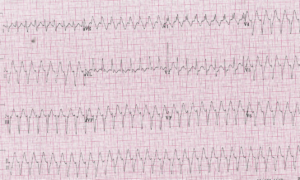
Working Diagnosis at time of Disposition:
Wide Complex Tachycardia: Ventricular Tachycardia vs SVT with aberrant conduction
ED & Hospital Course
Patient noted to be on 240 mg PO verapamil daily at home. Decision made to give Verapamil 5 mg IVP x 1. Patient immediately converted to Sinus rhythm at a rate of 100 bpm. Patient seen by both OB and EP at bedside. Electrolytes and troponin WNL. Normal Echo from 01/2019. Patient ultimately d/c with close f/u. Advised by EP to take extra ½ dose of Verapamil PO if palpitations recurred at home. Synthroid
discontinued.
Pearls & Takeaways
Diagnosis: Idiopathic Ventricular Tachycardia AKA Fascicular VT AKA Verapamil-sensitive VT AKA Belhassen-type VT
• Behaves like a reentrant tachycardia – usually seen in young adults (aged 15-40) w/o any structural heart disease (thus the term idiopathic)
• Mainly affects males (60-80% of cases)
• Fascicular VT is the most common idiopathic VT arising from the LEFT ventricle (thus the term fascicular)
• Most have QRS only modestly prolonged (~120-140ms) and fast initial forces (RS interval 60-80 ms)
• QRS relatively “narrow” due to the origin of the tachycardia being very early in the His-Purkinje system.
• Classified based on the site of origin/EKG morphology
o Posterior fascicular VT (95% of cases) – RBBB + LAD
o Anterior FT (5%) – RBBB + RAD
o Upper septal FT (very rare) – narrow QRS with RBBB
• OFTEN misdiagnosed as SVT with a RBBB – presence of capture or fusion beats indicates it is a ventricular tachycardia
• Usually stable despite high ventricular rates (>200/min)
• Will not respond to vagal maneuvers, adenosine, etc
• Belhassen et al first described its sensitivity to Verapamil
• Treatment: VERAPAMIL 2.5-10mg IVP (thus the term verapamil-sensitive VT)
• If you are uncertain of the diagnosis, first line treatment is synchronized cardioversion.
Reviriego S. Idiopathic fascicular left ventricular tachycardia. European Society of Cardiology 2010; 9 (13)
Belhassen B, Rotmensch HH, Laniado S. Response of recurrent sustained ventricular tachycardia
to verapamil. Br Heart J 1981; 46: 679-82.