
CC Chest pain and palpitations
HPI Pt is a 23 y/o male with no PMHx presenting with c/o palpitations, chest pain since last night. Pt states the pain is localized to the mid sternal chest wall with radiation to b/l upper extremities at times. Pt states the pain came on suddenly last night and he didn’t think anything of it so he went to bed. He woke up this morning with same pain and now with associated nausea and dizziness prompting the visit to the ED. Pt has never had pain like this in the past. Denies vomiting, F/C, recent illness, sudden cardiac death in the family other than a 70 y/o uncle who was obese. Pt denies drug use and states he was drinking over the weekend 2 days ago.
PMHx: none
Meds: none
Allergies: none
PSHx: none
Social: occasional ETOH, (-) drugs
Pertinent PE and Vitals: BP 90/62 P 186 RR 22 O2 sat 100% RA
General: Awake, alert, mild distress Cardiac: (+) tachycardic; no murmurs Lungs: CTAB, no rales, no rhonchi, no wheezing Abd: soft, nontender, nondistended Skin: diaphoretic; mild pallor
Pertinent Labs (if any) Troponin: 0.439
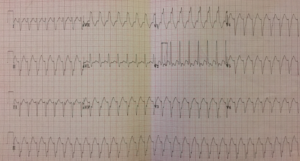
DDX: SVT with aberrancy vs VTach
ED Course: Pt placed on cardiac monitor immediately and IVF bolus initiated. Adenosine 12 mg IVP given while rhythm strip running with no change. A second dose of Adenosine 12 mg IVP given again with no change. 150 mg Amiodarone given with improvement of HR from 190’s to 170’s still wide complex. Second dose of 150 mg Amiodarone given with improvement of HR from 170‘s to 150’s and eventually converted to a NSR rate 85. Pt remained in stable condition and BP responsive to IVF. Pt admitted to telemetry and Cardiology consulted. While still in the ED, pt reverted back to wide complex tachycardia. 3rd dose of 150 mg Amiodarone given and recommendation from Cardiology was to try a 20 mg IVP of Cardizem. Cardizem given and pt immediately converted to NSR. Pt started on Cardizem drip and upgraded to the CCU. Pt underwent EPS and AV dissociation was noted. Determination was Verapamil Sensitive Ventricular Tachycardia. Pt remained stable throughout hospital course and started on Verapamil. Discharged on hospital day #3 with follow up with cardiology clinic.
Final Dx: Idiopathic Fascicular Left Ventricular Tachycardia AKA • Fascicular Tachycardia • Verapamil-sensitive VT • Belhassen-type VT
Discussion: MC type of idiopathic tachycardia of LEFT ventricle ! It is a reentrant tachycardia typically seen in young patients without structural heart disease ! Verapamil is first line treatment • Dose: 10 mg IVP over 1 minute ! EKG features: • Monomorphic V tach • QRS 100-140 ms (narrower than other forms of Tach) • Short RS interval 60-80 ms • RBBB pattern • Axis deviation depends on anatomical site of re-entry circuit ! Often misdiagnosed as SVT with RBBB ! Keys to dx: • Observe features of VT such as caption/fusion beats, AV dissociation • Usually unresponsive to adenosine, vagal maneuvers, or beta blockers
Post by: Kristen Pena, DO